
Add a video
MODULE 1
Anatomy, Assessment, and Clinical Implications
As body workers, and well practitioners, mastering the complexities of temporomandibular joint dysfunction offers a remarkable opportunity to provide relief for clients suffering from one of the most common and debilitating conditions affecting the cranial system. This is training helps you specialize in a niche that applies to many people today and take your treatment to a deep level.
In this first lesson we will establish the foundations needed to effectively address jaw pain, facial tension, and related symptoms through a comprehensive understanding of TMJ mechanics, assessment protocols, and the interconnected nature of cranial-facial structures.
Learning Objectives
Master the functional anatomy of the temporomandibular joint and its relationship to the craniosacral system
Develop comprehensive assessment skills for identifying various TMJ dysfunctions and their origins
Understand the neurological implications of TMJ dysfunction and its effects on the entire craniosacral system
Learn to differentiate between various causes of jaw pain and facial tension
Establish effective communication frameworks for discussing TMJ issues with clients
Create a foundation for applying specific TMJ treatment protocols
Functional Anatomy of the Temporomandibular Joint Complex
The temporomandibular joint represents one of the most complex and frequently used joint systems in the human
body. To effectively address TMJ dysfunction, practitioners must understand not only the structural components
but also the dynamic interrelationships that make this area particularly vulnerable to dysfunction.
Key Anatomical Structures
The Joint Components
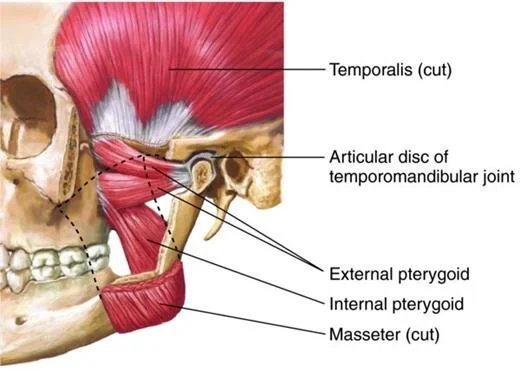
The temporomandibular joint is classified as a ginglymoarthrodial joint—a term that reflects its unique capacity for
both hinge-like (ginglymoid) and gliding (arthrodial) movements. This dual functionality allows for the complex movements required during speaking, chewing, and facial expression. Unlike many joints in the body, the TMJ contains a specialized articular disc that divides the joint space into superior and inferior compartments. This fibrocartilaginous disc serves as a crucial cushion between the mandibular condyle and the temporal bone’s articular surface, accommodating the differential movements that occurs during function.
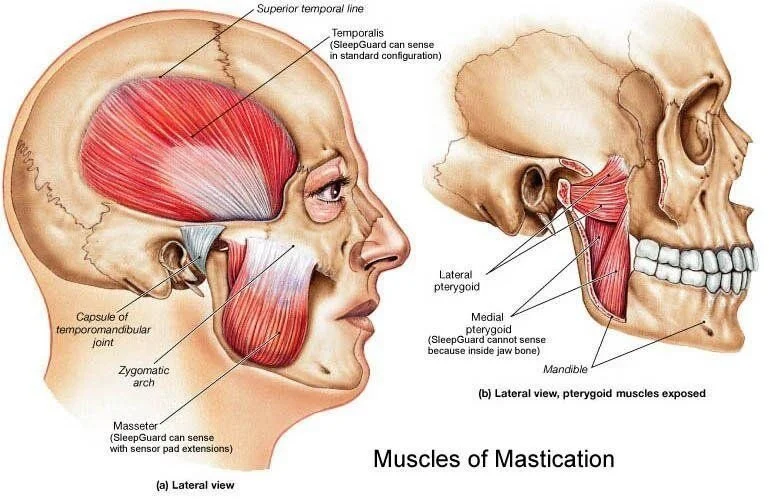
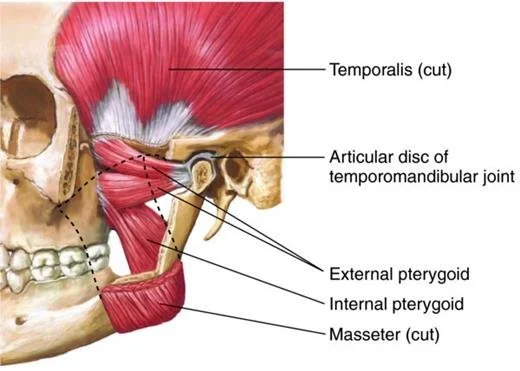
The TMJ function depends on a sophisticated coordination of multiple muscle groups: masseters, temporalis, medial pterygoid, lateral pterygoid, digastric, stylohyoid
Muscle Group
Masseter : Powerful jaw closure, elevation of mandible
Significance in TMJ Dysfunction: Often holds excess tension in bruxism; primary contributor to jaw clenching and related pain
Temporalis: Elevates and retracts mandible
Significance in TMJ Dysfunction : Frequent site of tension headaches related to TMJ dysfunction; affects temporal bone mobility
Medial Pterygoid: Elevates and protrudes mandible
Significance in TMJ Dysfunction : Deep tension affects internal joint mechanics; difficult to access directly
Lateral Pterygoid: Opens jaw, protrudes mandible, facilitates lateral movements
TMJ Dysfunction : Critical in disc displacement issues; dysfunction can lead to clicking/popping
Digastric : Assists in opening jaw and swallowing
TMJ Dysfunction: Influences hyoid position and therefore entire fascial chain connections
Stylohyoid: Elevates and retracts hyoid bone
TMJ Dysfunction: Creates compensatory patterns affecting throat and neck
The fascial system creates significant connections between the TMJ and distant body regions. Understanding these relationships allows practitioners to recognize how:
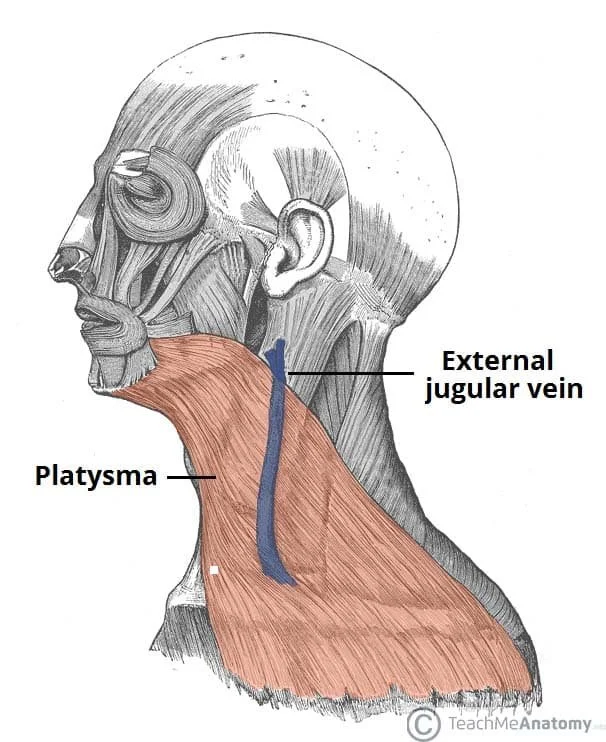
The superficial cervical fascia connects jaw tension to neck and shoulder dysfunction
The stylomandibular ligament creates a tension relationship between the cranial base and mandible
The buccopharyngeal fascia links TMJ function to throat and swallowing mechanisms
The masticatory fascia encapsulates the temporalis and masseter, creating a functional unit that affects cranial motion
Neurological Components
The trigeminal nerve (CN V) provides the primary sensory and motor innervation to the TMJ region, with
contributions from facial (CN VII), glossopharyngeal (CN IX), and accessory (CN XI) nerves for associated
musculature. This complex neural network explains why TMJ dysfunction can manifest with varied symptoms
including:
Facial pain and numbness
Ear symptoms (pain, fullness, tinnitus)
Headaches (particularly temporal and occipital)
Referred pain to neck and shoulders
Altered bite sensation and function
Biomechanical Function and Dysfunction
The TMJ performs three fundamental movement patterns that practitioners must understand to effectively assess dysfunction:
1. Rotation
The initial phase of mouth opening involves rotation of the mandibular condyle within the inferior joint space, allowing approximately the first 25mm of mouth opening. Restrictions in this rotational capacity often present as limited opening without deviation.
2. Translation
As mouth opening progresses beyond the rotational phase, the condyle-disc complex slides forward and downward along the articular eminence. This translation movement enables the full range of opening. Dysfunction in this phase typically manifests as deviation during opening or closing.
3. Lateral Excursion
The ability to move the jaw side to side involves complex coordination between the rotating condyle on the working side and the translating condyle on the balancing side. Restrictions in lateral movement often indicate muscle imbalance or disc displacement issues.
Primary Dysfunction Patterns
TMJ dysfunction typically presents in several key patterns that craniosacral practitioners should recognize:
1. Muscle-Dominant Dysfunction: Characterized by hypertonicity of masticatory muscles, often related to stress, clenching, or bruxism. Presents with diffuse pain, fatigue with chewing, and normal range of motion with discomfort.
2. Internal Derangement: Involves displacement of the articular disc, often presenting with clicking, popping, or locking. The disc may be displaced anteriorly, medially, or laterally, creating mechanical interference with normal movement.
3. Inflammatory Conditions: Including capsulitis, synovitis, or retro discitis, these conditions present with localized joint pain, swelling, and warmth. May result from trauma, overuse, or systemic inflammatory conditions.
4. Degenerative Changes: Arthritic changes to the joint surfaces present with crepitus (grating sounds), progressive limitation in movement, and pain that worsens with function and improves with rest.
Hypermobility/Instability: Excessive joint mobility leading to subluxation or dislocation. Often presents with jaw “catching” during wide opening or spontaneous dislocation events.
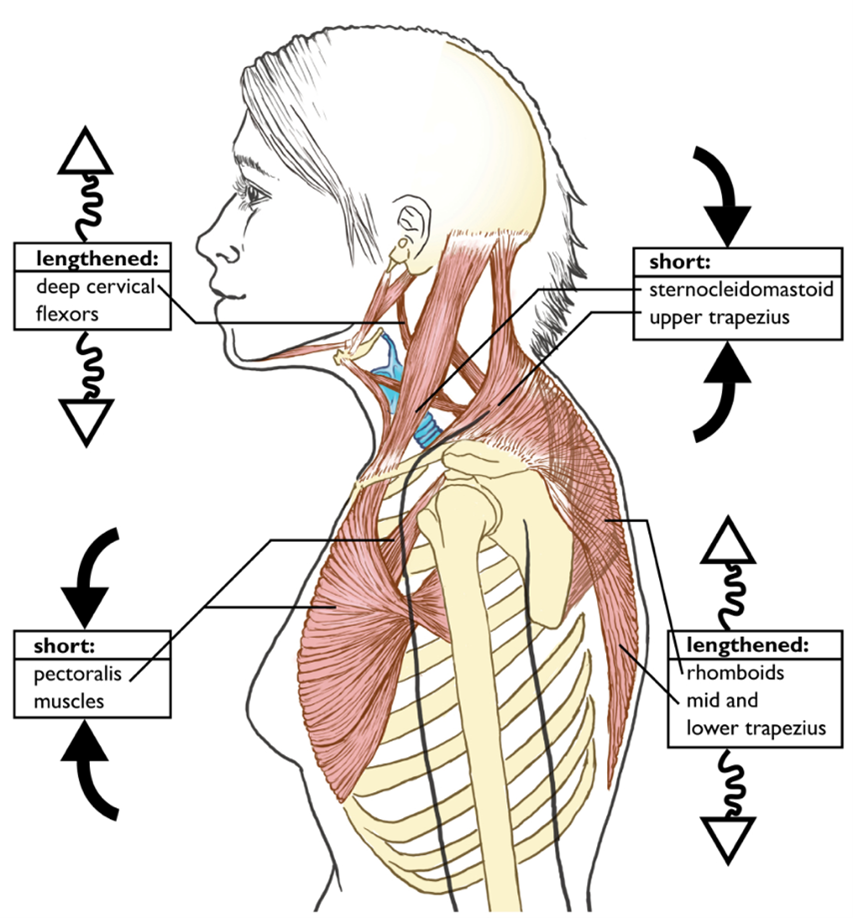
Your posture is a key player in the TMJ-cervical spine relationship. Poor posture, especially from prolonged, slumped sitting, mobile screen or TV use, or poor sleeping positions, can often lead to the following poor posture:
Forward head, poking chin posture, which shifts the jaw backward into a compressed position.
Rounded shoulders, which alters muscle recruitment patterns in the shoulders and upper back.
Increased tension in the upper trapezius muscles (large muscle across the top of your shoulders/lower neck) and suboccipital muscles (muscles at the base of your skull), which can lead to jaw clenching and headaches.
Altered tongue posture, affecting jaw alignment and breathing patterns.
This misalignment places excessive load on the TMJ and neck muscles, which can lead to pain, dysfunction, and reduced range of motion.
The temporomandibular joint holds a unique position within the craniosacral system, functioning as both an influencer of and responder to cranial bone motion. Understanding these interrelationships is essential for effectively addressing TMJ dysfunction through craniosacral approaches.
Temporal Bone Relationships
The temporal bone houses the mandibular fossa and articular eminence that articulate with the mandibular condyle. The temporal bone’s motion directly influences TMJ function:
External Rotation: The temporal bone’s external rotation during cranial flexion phase widens the mandibular fossa, potentially relieving compression on the TMJ structures.
Internal Rotation: During cranial extension phase, the temporal bone’s internal rotation narrows the mandibular fossa, which may exacerbate compressive symptoms in TMJ dysfunction.
Restrictions in temporal bone mobility—whether from cranial base compression, ear infections, or trauma—directly impact TMJ function. When assessing TMJ dysfunction, practitioners must always evaluate temporal bone mobility and position.
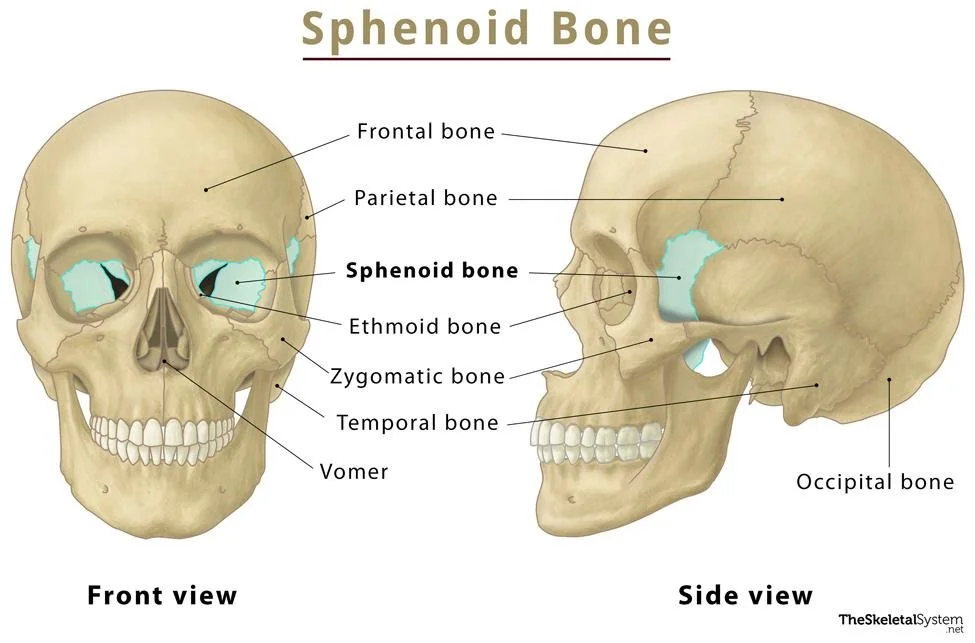
Sphenoid Influences
The sphenoid bone’s position and motion affect TMJ function through several mechanisms:
The lateral pterygoid plate of the sphenoid provides attachment for the lateral pterygoid muscle, a primary mover of the TMJ
Sphenobasilar junction (SBJ) patterns directly influence the position of the temporals and therefore the articular surfaces of the TMJ
Sphenoid torsion patterns often correspond with asymmetrical jaw function and unilateral TMJ symptoms
When addressing TMJ dysfunction, practitioners should always assess sphenoid position and mobility as part of a comprehensive evaluation.
Occiput and Upper Cervical Connections
The relationship between the TMJ, occiput, and upper cervical spine creates a functional complex where dysfunction in one area frequently affects the others:
The stylomandibular ligament connects the styloid process (temporal bone) to the angle of the mandible, creating a direct fascial link between cranial base and jaw
The rectus capitis muscles connect the occiput to the upper cervical spine, and their tone is often reciprocally related to masticatory muscle tension
The trigeminal-cervical nucleus in the brainstem allows for the neurological convergence of sensory information from both the TMJ and upper cervical regions, explaining referred pain patterns between these areas
Hyoid System Integration
The hyoid bone serves as a critical link between the TMJ, cranial base, cervical spine, and thoracic inlet. This floating bone, suspended by muscles and fascia, creates a tension network that influences and responds to TMJ
function:
The suprahyoid muscles (digastric, stylohyoid, mylohyoid, geniohyoid) connect the hyoid to the mandible and cranial base
The infrahyoid muscles (sternohyoid, omohyoid, thyrohyoid, sternothyroid) connect the hyoid to the sternum, scapula, and thyroid cartilage
Dysfunction in the hyoid system can manifest as throat tightness, swallowing difficulties, voice changes, and referred pain to the TMJ region
Assessment and treatment of the hyoid system is an essential component of comprehensive TMJ care within the craniosacral approach.
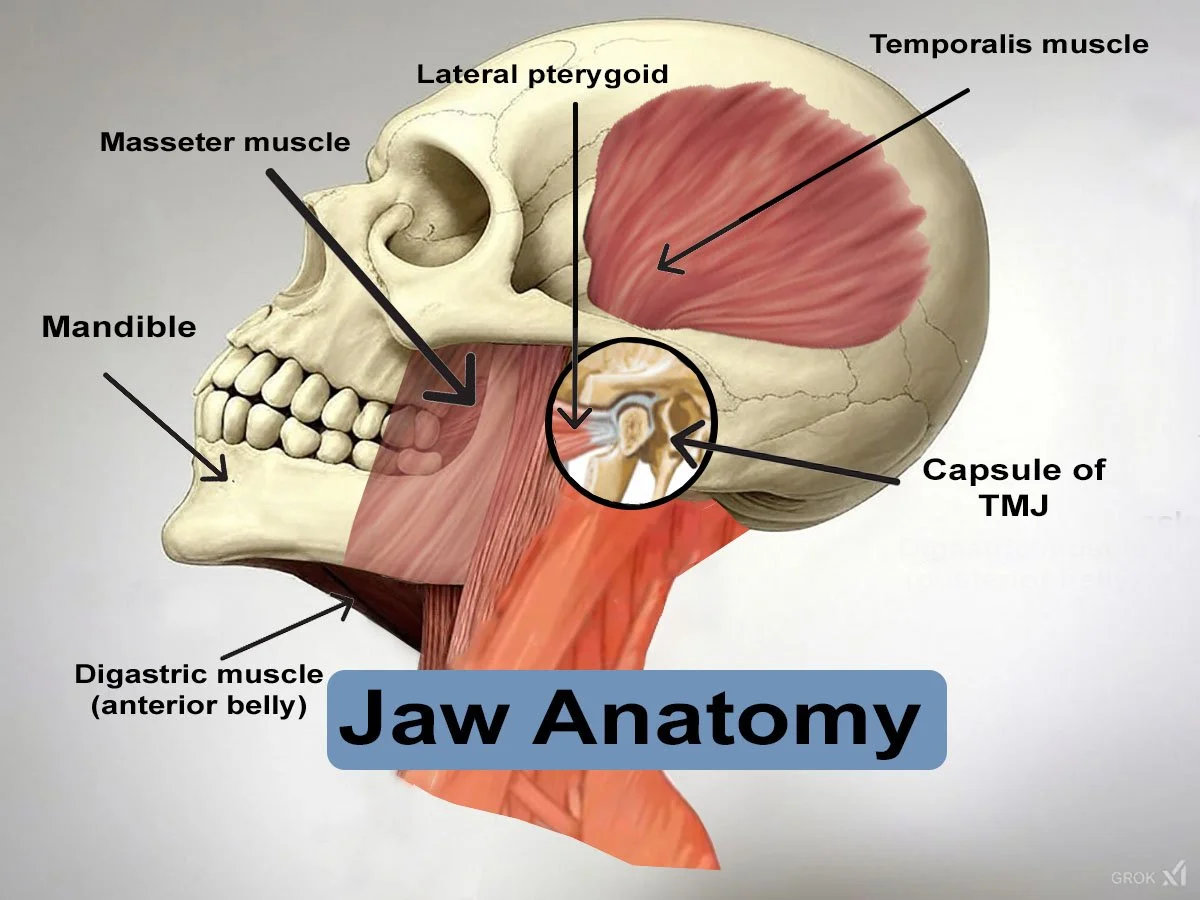
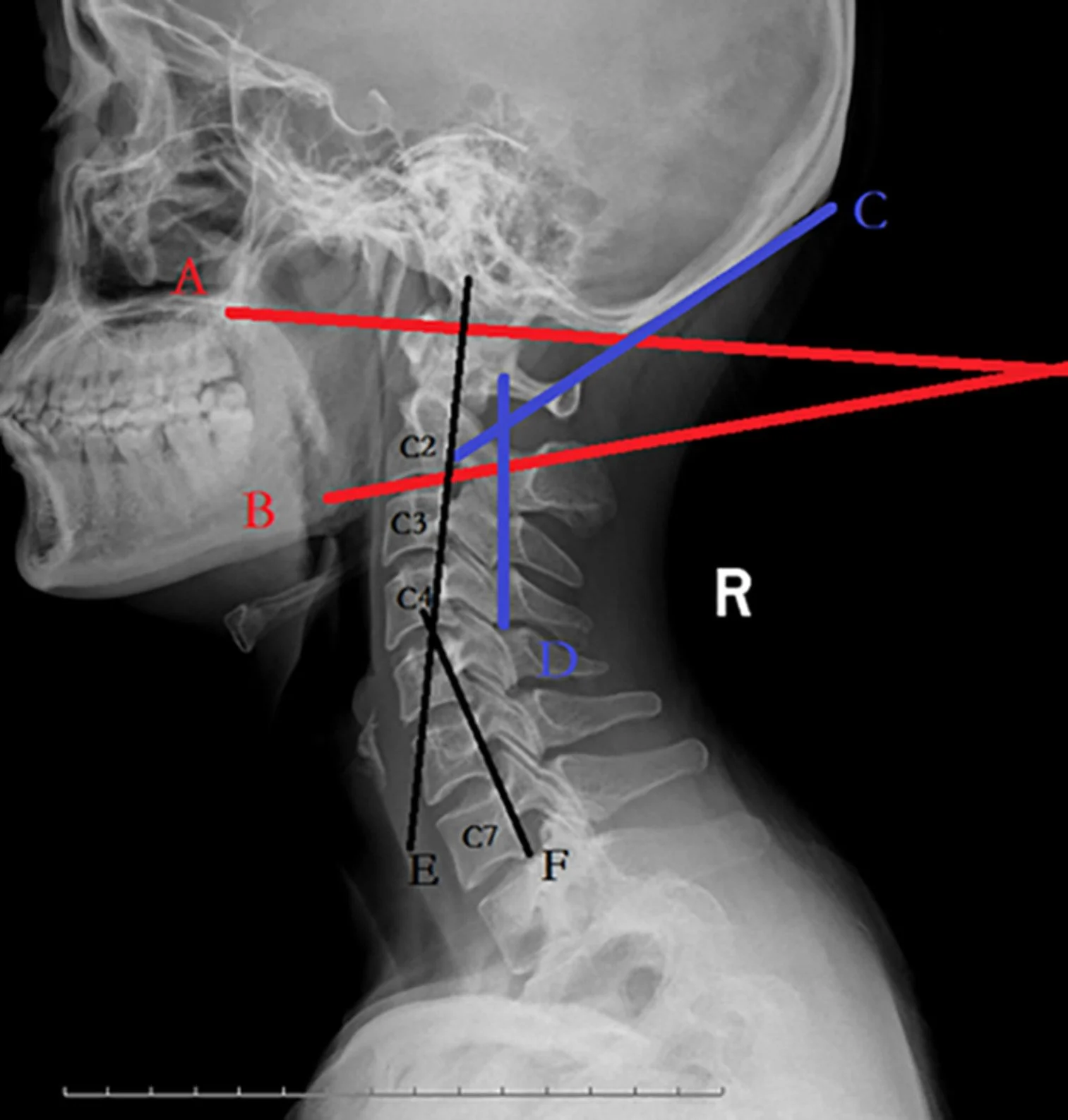
Cervical postural disorders can cause jaw pain. The anterior belly of the digastric muscle runs from the point of the chin to hyoid bone. This attachment means that when the head is protracted forward digastric will exert a posterior force on the mandible. With prolonged cervical protraction as occurs with poor posture or stress-related posture the mandibular condyle is pushed back against the retrodiscal tissue, eventually causing swelling, pain and gradual degeneration of the disc.
Comprehensive Assessment of TMJ Dysfunction
A thorough assessment forms the foundation for effective TMJ treatment. As a craniosacral practitioner, your
evaluation should integrate conventional TMJ assessment with craniosacral system evaluation to develop a
complete understanding of the dysfunction pattern.
Client History Components: The client interview should elicit specific information relevant to TMJ dysfunction. Key questions include:
Pain Characteristics:
Where exactly is your pain located?
Does it change location throughout the day?
How would you describe the quality of pain (sharp, dull, achy, throbbing)?
What is the intensity on a scale of 0-10?
When did you first notice these symptoms?
This differentiates muscle pain from joint pain; helps identify referred pain patterns; establishes baseline for tracking progress.
Functional Limitations:
Do you experience difficulty opening your mouth?
How wide can you open comfortably?
Is there any clicking, popping, or locking of your jaw?
Do you have difficulty chewing certain foods?
Has your bite changed or felt “off” recently?
This indicates severity of dysfunction; helps identify internal derangement; establishes functional impact of condition.
Behavioral Factors:
Are you aware of clenching or grinding your teeth?
Has anyone told you that you grind your teeth during sleep?
Do you frequently chew gum or bite on objects (pens, nails)?
Do you tend to hold tension in your jaw during stress?
This identifies contributing habits that must be addressed for successful outcomes; establishes behavioral modification needs.
Associated Symptoms:
Do you experience headaches? Where are they located?
Have you noticed any ear symptoms (pain, ringing, fullness)?
Do you have neck or shoulder pain that seems related?
Any symptoms of dizziness or balance issues?
Have you noticed any changes in your hearing or vision?
This establishes scope of craniosacral involvement; helps differentiate primary TMJ issues from referred symptoms; identifies need for medical referral.
Medical History:
Have you had any injuries to your head, face, or neck?
Have you had orthodontic work or major dental procedures?
Do you have any diagnosed conditions like arthritis, fibromyalgia, or other pain disorders?
What treatments have you tried for TMJ issues in the past?
This establishes potential contributing factors; identifies contraindications; helps determine need for interdisciplinary care.
Physical Assessment Protocols
A comprehensive physical assessment combines observation, palpation, and functional testing to establish the
precise nature of the TMJ dysfunction. The following protocol provides a systematic approach:
1. Observational Assessment
Facial Symmetry: Note any asymmetry in jaw position, muscle development, or overall facial balance.
Resting Jaw Position: Observe whether the jaw rests in a neutral position or shows deviation to one side.
Dental Occlusion: Note visible malocclusion, wear patterns on teeth, or obvious dental issues.
Postural Integration: Observe relationship between jaw position and head/neck posture.
2. Range of Motion Assessment
Assess the following movements, noting range, quality, and presence of pain or sounds:
Mouth Opening: Normal range is 35-50mm (approximately 3 finger widths). Measure from upper to lower central incisors.
Jaw Deviation: Observe whether the jaw deviates during opening and closing movements.
Lateral Excursion: Normal range is 8-12mm to each side.
Protrusion: Normal range is 6-9mm forward movement of mandible.
Retrusion: Normal range is 3-4mm of posterior movement.
3. Palpation Assessment
Systematically palpate the following structures, noting tenderness, tissue texture changes, and asymmetries:
TMJ Joint Capsule:
Place fingertips just anterior to the ear canal and have client open and close mouth; feel for movement, clicks, crepitus joint capsule tenderness suggests capsulitis; clicking indicates potential disc displacement; crepitus suggests degenerative changes.
Masseter Muscle:
Palpate from zygomatic arch to angle of mandible with flat palpation and pincer grip.
Hypertrophy suggests bruxism; trigger points may refer pain to teeth, maxilla, or ear.
Temporalis Muscle:
Palpate the fan-shaped muscle above the ear along the temporal fossa.
Trigger points commonly refer pain to upper teeth, eyebrow, or temple region; often involved in tension headaches.
Medial Pterygoid:
Intraoral palpation along medial surface of mandibular ramus (gloved finger).
Tenderness suggests deep masticatory tension; often involved in limited opening.
Lateral Pterygoid
Intraoral palpation behind maxillary tuberosity (gloved finger) .
Often involved in disc displacement issues; tenderness correlates with clicking and deviation.
Hyoid System:
Gentle palpation of hyoid bone and suprahyoid/infrahyoid muscles.
Restricted mobility suggests compensatory patterns affecting throat and neck.
4. Craniosacral Assessment Integration
Integrate specific craniosacral assessments to understand how TMJ dysfunction relates to the broader craniosacral
system:
Cranial Rhythm Evaluation: Assess quality, amplitude, and symmetry of craniosacral rhythm at the cranial base and mandible.
Temporal Bone Assessment: Evaluate for restrictions in external/internal rotation patterns.
Sphenoid Assessment: Check for torsion, side-bending, or compression patterns affecting the cranial base.
Dural Tube Tension: Assess for tension patterns in the dural system that may be influencing or responding to TMJ dysfunction.
Direction of Energy Evaluation: Determine the primary restrictions in the system that may be maintaining the TMJ dysfunction pattern.
Specialized Tests for TMJ Dysfunction
Several specialized tests can provide additional information about specific TMJ dysfunction patterns:
1. Load Testing
Apply gentle compression through the mandible with the mouth slightly open, then have client slowly close.
2. End-Feel Assessment
At the end range of mouth opening, apply gentle overpressure to assess tissue resistance:
Soft End-Feel: Normal muscular limitation
Hard End-Feel: Suggests internal joint blockage or bony restriction
Empty End-Feel: Client stops before tissue resistance due to pain – suggests acute inflammation
3. Joint Play Assessment
With client relaxed, gently mobilize mandible in various directions to assess quality of joint play movement.
Restricted movement suggests capsular tightness or adhesions.
4. Provocation Tests
Have client perform specific movements or functions to reproduce symptoms:
Sustained Opening: Holding wide opening for 30 seconds may reproduce pain in muscular disorders
Clenching: Sustained clenching may reproduce pain in muscular tension disorders
Chewing Simulation: Lateral grinding movements may reproduce symptoms in disc disorders
Decision-Making Framework for TMJ Dysfunction
A critical skill for addressing TMJ dysfunction is the ability to differentiate between various presentations and select appropriate treatment approaches. The following framework provides a systematic approach to assessment and treatment selection.
Classification of TMJ Dysfunction Patterns
The first step in effective treatment selection is proper classification of the dysfunction pattern. The following table outlines the primary categories of TMJ dysfunction and their distinguishing characteristics:
Muscular Tension Dominant:
Diffuse pain over masticatory muscles
Pain increases with function
Normal range of motion with pain at end ranges
Often bilateral symptoms
Morning jaw stiffness,
Tension headaches
Normal joint sounds
History of stress/tension habits
Treatment : Myofascial release techniques , Stress reduction strategies , Behavioral modification, Intraoral work like Buccal as tolerated.
Disc Displacement With Reduction:
Clicking/popping during opening, closing, or both
Deviation of jaw during opening that may self- correct
Normal or near- normal range of motion
Pain often localized to joint area
History of clicking for extended period
Intermittent catching sensation
Often unilateral symptoms
May have periods of no symptoms
Treatment: Lateral pterygoid release, Temporal bone balancing Joint decompression technique, Disc mobilization approaches
Disc Displacement Without Reduction:
Limited mouth opening (usually <30mm)
Deviation toward affected side during opening
History of clicking that suddenly stopped
Limited lateral movement away from affected side
Pain with attempts too pen wider
Sensation of blockage
Difficulty chewing
May have history of trauma or severe clenching
Treatment : Gentle decompression techniques, Cranial base normalization, Consider medical referral, Focus on symptom management.
Inflammatory Conditions:
Constant localized pain at joint
Pain dramatically increases with movement
Possible warmth or swelling
Recent onset or traumatic event
Pain at rest
Possible systemic inflammation
Morning stiffness
Treatment: Extremely gentle indirect techniques, Cranial work away from the joint, Medical referral as appropriate
Hypermobility/Instability:
Excessive range of motion (>50mm opening)
History of jaw dislocation
Fear of opening too wide
Joint may “catch” during movement
Often bilateral
May have generalized joint hypermobility
Muscular compensation patterns
Anxiety about joint function
Treatment : Stability- focused approaches, Proprioceptive training, Balance surrounding muscular support, Avoid further mobilization
Treatment Selection Flowchart
The following decision-making process guides practitioners through the selection of appropriate treatment approaches based on assessment findings:
1. Initial Assessment
Determine primary dysfunction pattern (muscular, disc displacement, inflammatory, hypermobility)
Assess contributing craniosacral patterns (temporal bone restrictions, sphenoid patterns, dural tension)
Evaluate systemic influences (stress levels, sleep quality, postural habits)
2. Safety Screening Decision Points
Is medical evaluation needed before proceeding? (acute trauma, neurological symptoms, systemic inflammation signs)
Are there contraindications to direct TMJ work? (acute inflammation, recent surgery, malignancy)
Is the condition within scope of practice? (minor displacement vs. severe dislocation)
3. Approach Selection Criteria
If primarily muscular tension: Begin with external muscle release approaches
If disc displacement with reduction: Focus on decompression techniques and lateral pterygoid release
If disc displacement without reduction: Use gentle cranial balancing and consider medical referral
If inflammatory: Use indirect techniques and distant work until acute phase resolves
If hypermobility: Emphasize proprioceptive approaches and stability training
4. Technique Selection Factors
Client comfort and tolerance for intraoral work
Practitioner skill level with specific techniques
Previous response to similar interventions
Acute vs. chronic nature of condition
5. Sequencing Decision
Begin with cranial base normalization to create supportive foundation
Address primary restrictions in temporal bones before direct TMJ work
Progress from gentle, indirect techniques to more direct approaches as tolerated
Integrate self-care strategies throughout treatment process
Comparative Analysis of Treatment Approaches
The following table compares different treatment approaches for TMJ dysfunction, helping practitioners select the most appropriate techniques based on specific client presentations:
Myofascial release : effective for muscular tension patterns, stress related bruxism, clients new to body work, facial pain with radiation. This does not access deeper structures, only temporary relief.
Intraoral/ buccal techniques: effective for pterygoid muscle tension, restricted jaw mobility, deep fascial restriction, trigger points that cant be accessed externally. Requires hygiene protocols, may trigger gag reflex, ineffective for clients with acute inflammation.
Cranial Base Techniques: effective for TMJ dysfunction with cranial bone restriction, headaches, complex pain patterns involving multiple cranial areas, creating foundational balance before TMJ work. This requires client understanding of subtle work, doesn’t address specific mechanical joint in TMJ, must be used with TMJ work.
Joint Mobilization: effective for restricted joint, mild disc displacement with reduction, hypo mobility. Not appropriate for hyper mobility, requires precise application , and is a bit uncomfortable for client.
Hyoid & Throat: effective for swallowing issues, voice changes , forward head posture issues, tension in throat. requires careful approach, gentle, to be used as an integrative component to other approaches.
Client-Specific Considerations
Age Factors: Younger clients typically respond more quickly; older clients may have more complex, chronic patterns with degenerative changes requiring gentler approaches.
History Duration: Recent onset conditions typically respond more readily than long-standing dysfunction with established compensatory patterns.
Emotional Components: TMJ dysfunction frequently has emotional components (stress, anxiety, trauma)
that may require integration of nervous system regulation approaches.
Sleep Quality: Poor sleep often maintains or exacerbates TMJ issues, particularly nighttime bruxism, requiring specific sleep-related interventions.
Occupational Factors: Certain occupations (musicians, public speakers, dental professionals) place specific demands on the TMJ system and require tailored approaches.
Health Status Modifications
Inflammatory Conditions: Systemic inflammatory conditions (rheumatoid arthritis, psoriatic arthritis) require gentler approaches with emphasis on indirect techniques.
Neurological Conditions: Conditions affecting muscle tone or control (Parkinson’s, dystonia) necessitate modified approaches with emphasis on gentle facilitation rather than deep release.
Connective Tissue Disorders: Hypermobility syndromes (Ehlers-Danlos) require focus on proprioceptive training and stability rather than mobility enhancement.
Dental Status: Recent dental work, missing teeth, or malocclusion issues require coordination with dental professionals and modification of direct techniques.
Individualized Response Considerations
Tissue Responsiveness: Some clients display highly responsive tissue that changes quickly with minimal input; others require more sustained intervention for lasting change.
Pain Sensitivity: Clients with central sensitization or heightened pain responses require gentler approaches with gradual progression.
Psychosocial Factors: Client beliefs about their condition, previous healthcare experiences, and support systems significantly impact treatment responsiveness.
Case Studies: Decision-Making in Action
The following case studies demonstrate the application of the decision-making framework in different client scenarios, illustrating how a craniosacral practitioner might approach various presentations of TMJ dysfunction.
Case Study 1: Stress-Related Muscular TMJ Dysfunction
Client Presentation
Client: 42-year-old marketing executive
Primary Complaints: Bilateral jaw pain, morning stiffness, occasional headaches
Assessment Findings:
Normal range of motion (45mm opening) with pain at end range.
Significant masseter and temporalis hypertonicity bilaterally
No clicking or joint sounds
Reports high stress, deadline pressure, and jaw clenching awareness
Craniosacral evaluation shows restricted temporal bone mobility and compressed cranial rhythm
Decision-Making Process
1. Classification: Primary muscular tension pattern with stress-related bruxism
2. Safety Screening: No red flags; appropriate for full craniosacral intervention
3. Approach Selection:
Begin with external myofascial techniques
Address cranial base restrictions
Include temporal decompression
Add intraoral work as tolerated in later sessions
4. Personalization Factors:
High-stress profession requires emphasis on self-regulation strategies
Incorporate stress management education
Address sleep quality and nighttime bruxism
Treatment Plan
Initial Phase (Sessions 1-3):
Cranial base decompression to establish foundation
External masseter and temporalis release techniques
Temporal bone balancing protocol
Introduction to jaw relaxation exercises and stress awareness
Intermediate Phase (Sessions 4-6):
Addition of intraoral pterygoid release techniques
Hyoid release to address compensatory patterns
Refined home program with emphasis on daytime awareness
Introduction of self-massage techniques
Final Phase (Sessions 7-8):
Integration of full craniosacral rhythm balancing
Comprehensive stress management strategies
Sleep quality enhancement approaches
Maintenance plan with periodic check-ins
Outcome and Rationale
This approach addresses both the physical manifestations of TMJ dysfunction and the underlying stress factors driving the condition. Beginning with external techniques builds rapport before introducing more invasive intraoral work. Emphasis on self-care strategics provides sustainable results for this stress-driven pattern.
Practical Exercise: TMJ Assessment and Treatment Planning
Exercise: Developing TMJ Assessment Proficiency
This exercise will help you develop the assessment skills necessary to accurately classify TMJ dysfunction and develop appropriate treatment plans. You’ll need a practice partner for this exercise.
Part 1: Assessment Practice
1. With your practice partner, conduct a complete TMJ assessment following the protocols outlined in
this lesson:
Client history (using the key questions provided)
Observational assessment
Range of motion assessment
Palpation assessment
Craniosacral assessment integration
Specialized tests as appropriate
2. Document your findings using a systematic format that captures all relevant information.
3. Based on your assessment, classify the primary dysfunction pattern using the categorization system
presented in this lesson.
Part 2: Treatment Planning Exercise
1. Based on your assessment findings, develop a comprehensive treatment plan that includes:
Primary focus of treatment
Specific techniques selected
Sequence of interventions
Client education components
Home program recommendations
Present your treatment plan as if explaining it to the client, using accessible language while maintaining professional clarity.
Identify specific personalization factors that would modify your approach based on individual client factors.
submit your work to : VEDAWELLNESSCO@GMAIL.COM
Exercise Solution Guide
While each practice partner will present with unique findings, your assessment and treatment plan should demonstrate the following elements:
Assessment Documentation Example:
Client History: 35-year-old with 6-month history of right-sided jaw pain, occasional clicking, pain worse in mornings and during stressful periods. Reports teeth clenching awareness.
Observation: Slight asymmetry with right side appearing more developed/tense. Head positioned slightly forward with mild right rotation.
Range of Motion: Opening 38mm with deviation to right initially that corrects; right lateral excursion limited to 6mm (left 9mm); protrusion normal.
Palpation: Right masseter hypertonic with trigger points referring to upper teeth; right TMJ tenderness; moderate temporal muscle tension bilaterally.
Craniosacral Findings: Right temporal bone restricted in external rotation; compressed rhythm at cranial base; sphenoid in right torsion pattern.
Classification: Mixed presentation – muscular tension pattern with mild disc displacement with reduction (right side).
Treatment Plan Example:
Client Communication: “Based on today’s assessment, I’ve found that your jaw pain stems from two main factors working together. First, there’s significant tension in the muscles that control your jaw, particularly on the right side. This appears to be related to clenching, especially during sleep and stressful periods. Second, there’s a slight displacement of the disc in your right jaw joint that’s causing the clicking when you open and close.
“Our treatment plan will address both these issues through a step-by-step approach. Initially, we’ll focus
on releasing muscle tension and creating better balance in the cranial bones that form the foundation for your jaw joint. As treatment progresses, we’ll work more specifically on the joint mechanics and the deep muscles that control the disc position.”
“I recommend a series of 6-8 sessions, starting with weekly treatments and then spacing them out as we see improvement. Throughout the process, I’ll provide you with specific self-care techniques to support your progress between sessions.”
Treatment Sequence Rationale:
Begin with cranial base normalization to establish proper foundation for TMJ function
Address temporal bone restrictions to improve joint relationships
Release external musculature before progressing to deeper structures
Incorporate intraoral work once rapport and comfort established
Balance focus between structural corrections and self-management strategies
Personalization Factors:
Stress management strategies tailored to client’s specific stressors
Sleep position modifications based on habitual patterns
Consideration of occupational speaking demands in treatment progression
Adjustment of home care program to realistic time availability
Developing Clinical Reasoning for TMJ Dysfunction
As you develop your skills in assessing and treating TMJ dysfunction, the refinement of your clinical reasoning process becomes essential. This section explores the deeper thinking processes that guide effective clinical decision-making.
Beyond the Obvious: Recognizing Hidden Patterns
TMJ dysfunction rarely exists in isolation. As a skilled practitioner, your ability to recognize underlying patterns and connections will substantially enhance treatment outcomes:
Cranial Extension/Flexion Patterns: Observe whether TMJ dysfunction corresponds with broader cranial extension or flexion dominance, which influences treatment approach.
Reciprocal Tension Relationships: Identify how TMJ tensions create or respond to tensions elsewhere in the body, particularly cervical spine, shoulders, and pelvic positioning.
Developmental Origins: Consider whether TMJ patterns reflect early developmental movements or compensations that have become embedded in the system.
Breathing Patterns: Recognize how TMJ dysfunction often correlates with altered breathing mechanics, particularly mouth breathing or upper chest breathing patterns.
Autonomic Regulation: Observe the relationship between TMJ tension and autonomic nervous system state, noting how sympathetic activation often corresponds with increased jaw tension.
Integrating Multiple Assessment Systems
Sophisticated clinical reasoning involves synthesizing information from multiple assessment frameworks:
Biomechanical Assessment: Evaluating structural relationships and movement patterns
Biodynamic Assessment: Perceiving fluid dynamics and primary respiratory mechanism
Neurological Assessment: Understanding nervous system regulation and sensory processing
Psychosocial Assessment: Recognizing emotional and lifestyle factors influencing presentation
When these assessment frameworks are integrated, a more complete understanding of the client’s condition emerges, guiding more effective treatment planning.
The Art of Treatment Progression
Skilled clinical reasoning includes thoughtful decisions about treatment progression:
Reading Tissue Response: Develop sensitivity to how tissues respond to intervention, adjusting pressure, direction, and duration accordingly.
Recognizing Therapeutic Windows: Identify the optimal therapeutic challenge—enough to stimulate change but not so much as to trigger protective responses.
Following the Process: Allow the treatment to unfold according to the body’s priorities rather than imposing a predetermined sequence.
Integration Pauses: Recognize when to pause techniques to allow for integration of changes before proceeding further.
End-Point Recognition: Develop the discernment to recognize when a structure has reached optimal balance and further intervention would be counterproductive.
Adapting to Individual Variation
Perhaps the most advanced aspect of clinical reasoning is the ability to adapt general principles to individual client variations:
Tissue Quality Variations: Adjust techniques based on tissue density, hydration, and responsiveness.
Nervous System Sensitivity: Modify approach based on client’s sensory processing characteristics and autonomic regulation capacity.
Rate of Change Differences: Recognize that clients integrate changes at different rates and adjust treatment spacing accordingly.
Cultural and Personal Factors: Adapt communication and therapeutic approach to align with client’s cultural background and personal preferences.
By developing these deeper aspects of clinical reasoning, you transform from a technician following protocols to an
artful practitioner able to provide truly personalized care for TMJ dysfunction.
Summary and Integration
This lesson has established the essential foundations for understanding, assessing, and developing treatment
approaches for temporomandibular joint dysfunction. Through a comprehensive exploration of TMJ anatomy,
biomechanics, assessment protocols, and decision-making frameworks, you’ve developed the knowledge base
necessary for effective intervention.
Key concepts from this lesson include:
The complex anatomical and biomechanical nature of the TMJ and its relationship to the craniosacral system
Systematic assessment protocols that enable accurate classification of TMJ dysfunction patterns
Decision-making frameworks for selecting appropriate treatment approaches based on client presentation
The importance of personalization in developing effective TMJ treatment plans
Clinical reasoning processes that transform technique application into artful practice
In the next lesson, you’ll build upon this foundation by learning specific treatment protocols for TMJ dysfunction,
including external and intraoral techniques, cranial balancing approaches, and specialized protocols for different
dysfunction patterns. These practical skills will enable you to effectively address the full spectrum of TMJ issues in
your clinical practice.
Add a short summary or a list of helpful resources here.